Abortion is not development aid for mothers
Posted by Dan Blackman on 26 March 2012
SPUC recently held a very successful conference in London on the topic of abortion and maternal health in the developing world.
One of the key issues looked at was the funding given for promoting and doing abortions in the developing world. The Department for International Development (DFID) gives hundreds of millions to organisations like International Planned Parenthood Federation (IPPF), Marie Stopes International (MSI) and International Projects Assistance Services (Ipas) who specialise in killing unborn children. This funding usually takes the form of a Partnership Programme Arrangement (PPA) which lasts several years, but funding for individual and country-specific programmes can also be given under initiatives like the Civil Society Challenge Fund (CSCF).
The latest project launched by DFID is called Preventing Maternal Deaths from Unwanted Pregnancy (PMDUP). DFID will give £67 million pounds over 5 years from July 2011 to June 2016 via MSI and Ipas, to carry out and promote abortion and contraception in 14 countries: Afghanistan, Bangladesh, India, Myanmar, Pakistan, DRC, Ethiopia, Ghana, Malawi, Nigeria, Sierra Leone, Sudan, Zambia, and Zimbabwe. In its Business Plan (2011 - 2015) DFID committed ‘to embed in every relevant bilateral programme specific plans to take forward the promotion of choice for women over whether and when they have children’ - i.e. DFID will make sure abortion and contraception are part and parcel of any funding and aid they offer, as far as possible.
Reading through the PMDUP business plan reveals that MSI and Ipas will be responsible for collecting the programme data, and Options - the consultancy firm wholly owned by MSI - will provide consultancy for the PMDUP programme and be linked to the impact evaluation. Options will also be involved in providing evidence to shape PMDUP implementation strategy. Not only is DFID leading the way in killing unborn children in the developing world, they are getting the abortion organisations to collect the programme data for the programmes they themselves will be carrying out, provide consultancy to DFID, and influence the impact evaluation of the programme they have been asked to do.
To use an analogy, it's a bit like a firm making landmines being given tens of millions to make and plant landmines in the developing world, and allowing that same firm making the landmines to collect data on the impact of landmines, advise the government on the safety and effectiveness of their programme to promote landmines, and then allowing the firm to evaluate themselves. The mind boggles.
Some charts are provided in the business plan about "growth forecast" for the PMDUP programme. The 2 charts below detail the hoped for number of women having abortions and receiving contraceptive devices by MSI and Ipas. The second chart details the future increase in the number of MSI and Ipas facilities conducting abortions - usually using misoprostol or manual vacuum aspirators.
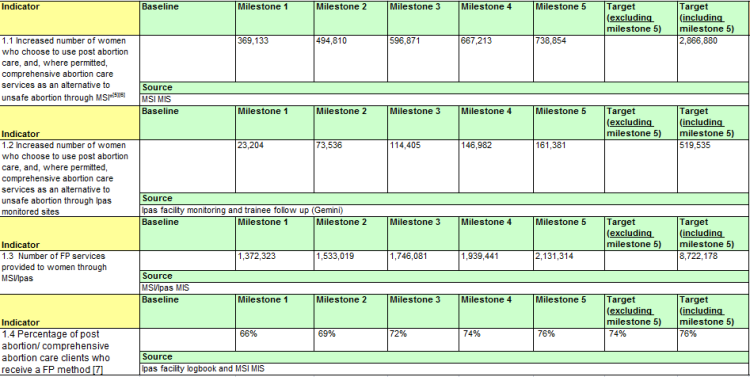
For MSI 2,866,880 mothers are expected to undergo an abortion or post-abortion "care", and for Ipas the figure is 519,535. It's very probable that Options or MSI and Ipas themselves came up with these figures, considering how much of a free rein they have been given by DFID.
The term "post abortion care" (PAC) is deceptive. PAC is part and parcel of the abortion promotion agenda of organisations like IPPF, WHO, DFID, MSI, and Ipas who in 1993 together with IPPF founded the PAC Consortium. In 2007 pro-lifers and religious leaders rejected proposals by the Guatemalan Ministry of Health to introduce post-abortion care into public health, citing the reason that such measures are tactics to further the abortion agenda.
One of the uses of PAC is getting the abortion drug misoprostol into countries for post-abortion and incomplete abortion "services", as seen from the PAC Consortium misoprostol resources pages of their website. The devastating effect of misoprostol on a developing country has already been presented by Dr Susan Yoshihara, following the 2010 Women Deliver Conference. Several years ago the World Health Organisation changed its policy to include misoprostol on its list of essential medicines. This move was supported by radical pro-abortion organisations such as Gynuity and MSI. This is noted by the pro-abortion Center for Reproductive Rights, and used as another prong to further abortion and avoid maternal morbidity and mortality.
PAC is a cover for introducing abortion into countries where it is illegal or highly restricted, as noted by Dr Ideh at the SPUC maternal mortality conference. We have also seen this recently in the case of Rwanda. The radically pro-abortion Guttmacher Institute produced a study citing the lack of post-abortion care as a reason for abortion-related morbidity and lack of family planning, always discussed and offered following an abortion, as reasons for liberalising Rwanda's law on abortion. Guttmacher is supporting the lobbying efforts of Rwanda's IPPF affiliate in the country. PAC is a useful cover, as it allows abortion organisations to train people, from doctors to community health workers, to conduct abortions using MVA and misoprostol, and promote contraceptive devices, better know as post-abortion family planning. It also reinforces the canard of safe v unsafe abortion by claiming that abortion is safe where post-abortion care for complications is easily available. PAC is part of a strategy which seeks to normalise abortion at the level of public opinion and medical consensus, and persuade legislators that a country's abortion laws need to be changed in favour of abortion.
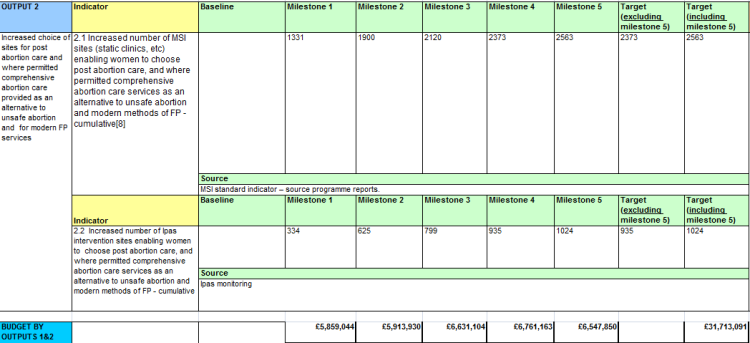
What this chart above sets out is the increased number of abortion and contraception facilities that MSI and Ipas hope to establish by 2016. The total for MSI is 2563 and 1024 for Ipas.
These are desperate times for mothers, babies, and families in the developing world, where our taxes are being used to kill unborn children and harm the health of mothers. Money is being diverted away from the real causes of maternal morbidity and mortality, and instead being used to serve the ideological agenda of DFID and its partners IPPF, MSI, and Ipas. We now live in a world where the manual vacuum aspirator in the hands of an abortionist counts as aid to developing countries.